Why IED Explosions Feel Instantaneous
When someone with IED has a verbal explosion over what seems like a minor trigger — a misheard comment, a small inconvenience, a slightly dismissive tone — onlookers often interpret this as a choice. As temper. As selfishness. What they don't see is what is happening inside the nervous system in the 300 milliseconds before the explosion.
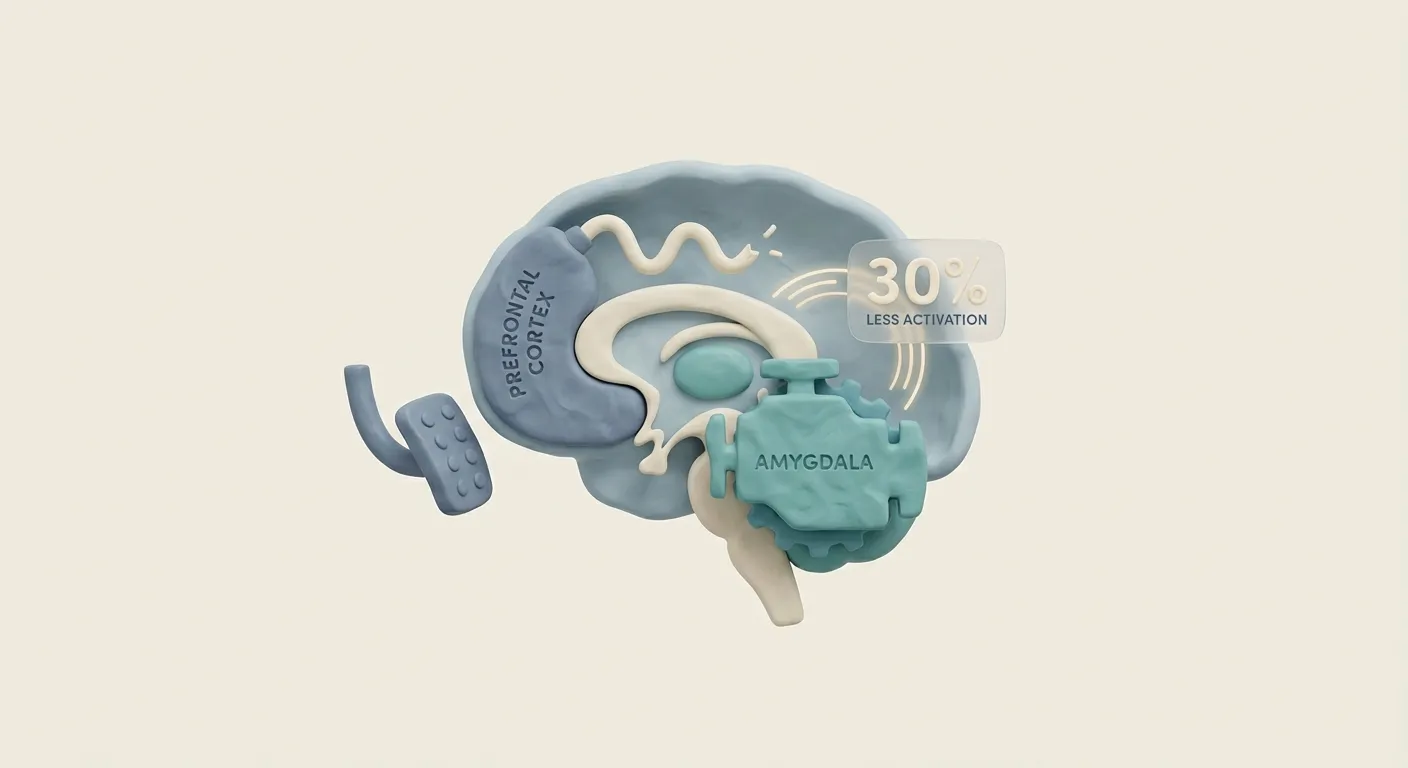
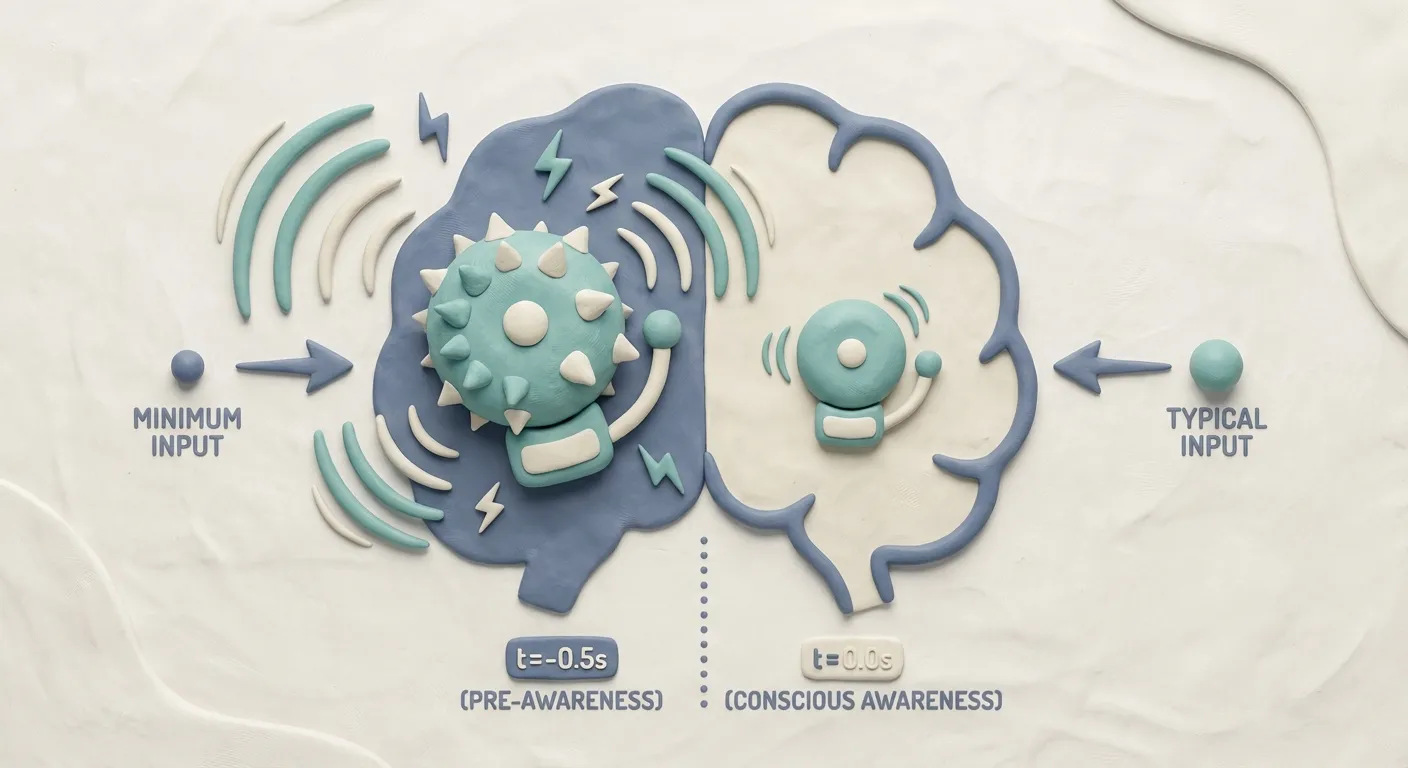
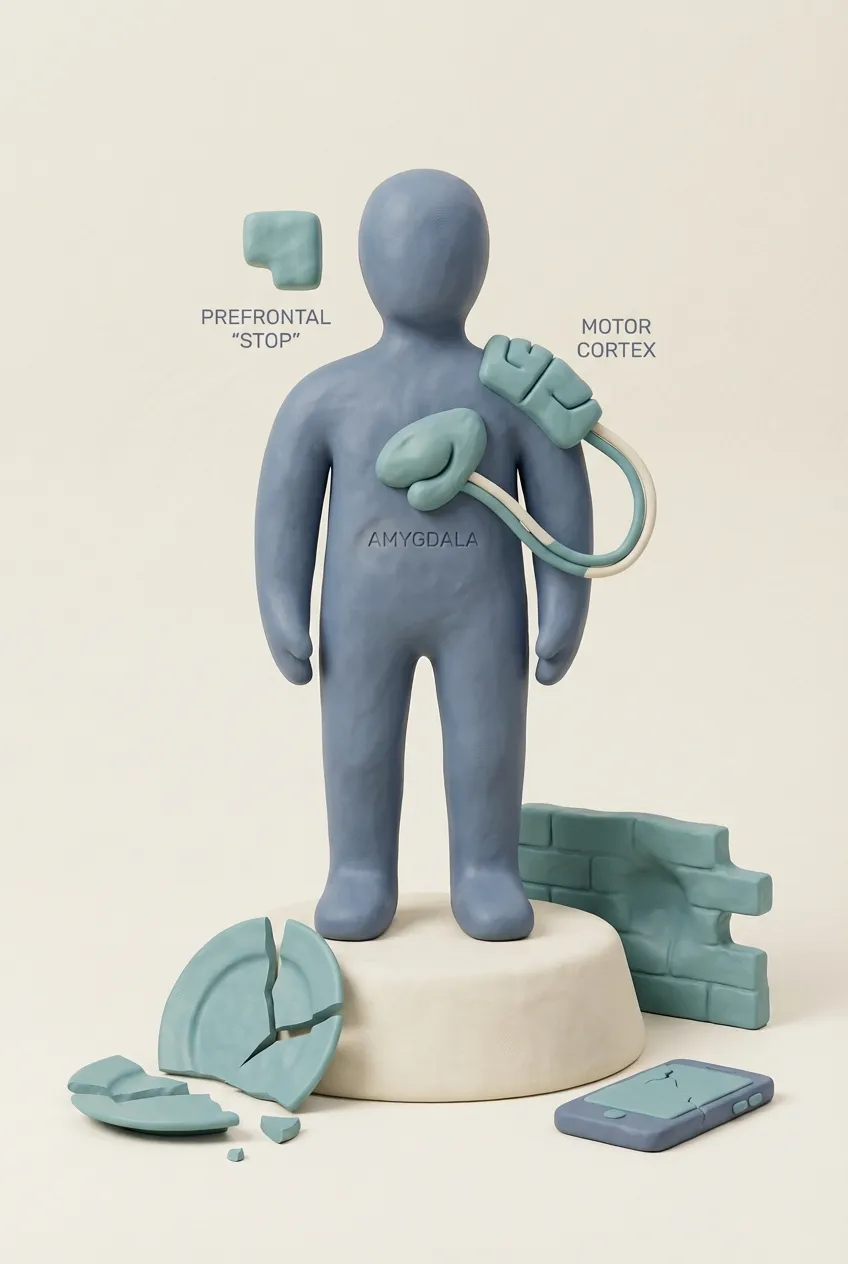
The amygdala — your brain's alarm system — processes sensory input and generates threat responses in approximately 300 milliseconds. In a neurotypical brain, the prefrontal cortex receives this signal and applies context, consequence evaluation, and behavioural inhibition in the following 300-600 milliseconds. This second phase is what we think of as 'thinking before acting.' In IED, this second phase is significantly delayed or underactivated. The alarm fires. The response launches. The thinking-it-through arrives too late.
This is not a metaphor. Neuroimaging studies show reduced prefrontal-amygdala connectivity in people with IED. The circuits that normally put the brakes on an alarm response are simply less engaged in the moment of trigger. The explosion feels instantaneous because, neurologically speaking, it nearly is.
People with IED often describe the experience as watching themselves from the outside — aware that something is happening, unable to stop it, almost as if they were passengers in their own reaction. This dissociative quality isn't weakness. It's a consequence of the speed at which the event unfolds.
Understanding this matters for two reasons. First, it removes the moral framing that makes this experience so isolating. You are not a bad person with bad values who chose to explode. You are a person whose neurological brake system engages too slowly for the speed of your alarm. Second, it points toward what actually helps: interventions that work at the level of early physical warning signs (before the explosion), not strategies that assume you can 'choose' your way out of it once it has begun.
Recovery from an episode typically happens within 20-30 minutes. Many people experience genuine calm, even euphoria, immediately after — not because they enjoyed it, but because the neurological storm has passed and the body is releasing counter-regulatory neurochemicals.
- The amygdala fires 300ms before the prefrontal cortex can apply brakes — the explosion is neurologically near-instantaneous.
- Reduced prefrontal-amygdala connectivity is measurable in IED — this isn't a choice or a character flaw.
- Many people experience dissociation during episodes, aware of but unable to stop their own reaction.
- Effective interventions target early physical warning signs — not willpower in the moment of explosion.
The Neuroscience of Explosive Tunnel Vision
One of the most disorienting aspects of IED — for the person experiencing it and for anyone trying to understand it from the outside — is the quality of tunnel vision that accompanies an episode. In the moment of explosion, the field of awareness collapses. The trigger becomes the entire world. Nothing else registers.
This is not selective memory or convenient forgetting. It is a documented feature of high-amygdala-activation states. When the brain's alarm system goes into emergency mode, it narrows attention to the perceived threat with extraordinary focus. This is an evolutionary feature, not a bug — in a genuine survival threat, you need every cognitive resource pointed at the danger, not distributed across context and consequence evaluation.
The problem is that IED activates this survival-mode tunnel vision in response to social and interpersonal triggers that are not, in fact, survival threats. A partner's sharp tone. A cashier's dismissive attitude. A driver cutting across your lane. These are not physically dangerous. But the amygdala, hyperreactive and running ahead of the prefrontal cortex's contextualising influence, processes them as if they were.
During this tunnel vision state, people with IED often report that they genuinely cannot access information they normally know very well. They cannot recall that this person loves them, that this will pass, that the relationship matters, that there will be consequences. This information is not deleted — it simply becomes inaccessible in the seconds during which the alarm state is driving behaviour.
What looks like disproportionality from the outside feels, from the inside, like a completely proportionate response to a very real and immediate threat. The discrepancy is not dishonesty. It is the gap between the amygdala's appraisal of the threat (extreme) and objective reality (minor inconvenience).
After the episode, context returns. So does deep confusion about what just happened, and shame about the response relative to the trigger. Understanding that this is the tunnel vision collapsing — not evidence that you are fundamentally dangerous — is an important part of building a realistic self-concept around IED.
- High amygdala activation collapses awareness to the trigger — context, consequences, and relationships become inaccessible in the moment.
- The tunnel vision is an evolutionary survival feature misfiring on non-threatening social triggers.
- What feels proportionate inside an episode looks wildly disproportionate from outside — both perceptions are neurologically real.
- When context returns after an episode, the confusion and shame are also genuine — not performance.
Why the Escalation Is So Fast
People who know someone with IED often say the same thing: 'There was no warning. One moment they were fine, then suddenly they weren't.' And for a long time, this observation was used to cast doubt on the sincerity of the calm. If you were truly fine, how could you be explosive so quickly? The implication was performance — manipulation — control that was available and withheld.
This framing is neurologically wrong, and it causes enormous harm.
The calm before a lightning-strike episode is genuine. The person with IED is not simmering, waiting, performing stillness. Their nervous system is actually in a relatively regulated state. And then a trigger arrives — something that the hyperreactive amygdala reads as threatening — and the transition from regulated to explosive happens in seconds, because the neurological pathway being activated is not the slow, deliberate cortical pathway. It is the fast subcortical alarm pathway.
Think of it like a circuit breaker versus a dimmer switch. Neurotypical emotional escalation tends to follow a dimmer-switch pattern — you can observe the buildup, modulate it, respond to de-escalation attempts along the way. IED escalation follows a circuit-breaker pattern: stable, stable, stable, TRIP. There is no intermediate state to catch and address. The switch has flipped.
This characteristic is actually one of the diagnostic criteria for IED — that the explosive episode is grossly out of proportion to the trigger and occurs rapidly. Research using ecological momentary assessment (measuring emotional states in real time across the day) confirms that IED episodes are genuinely abrupt, not the culmination of slow-building anger that the person was somehow concealing.
One of the most important things someone with IED can learn to notice is the physical precursor state that exists in the seconds before an episode. Even when the emotional escalation is too fast to catch, the body often has a few seconds of warning — a flush of heat, tension in specific muscle groups, a changed quality of breathing. Learning to recognise and respond to these physical cues is the primary access point for intervention, because the cognitive window is simply too short.
- The calm before a lightning-strike episode is neurologically genuine — not performance or concealed anger.
- IED follows a circuit-breaker pattern, not a dimmer-switch pattern — the switch flips, there is no observable slow buildup.
- Ecological momentary assessment research confirms IED episodes are genuinely abrupt, not disguised gradual escalation.
- Physical body cues (heat, muscle tension, breathing changes) are the primary window for early intervention.
The Shame That Follows the Storm
IED is often discussed in terms of the explosion itself. Less often discussed — and perhaps more consequential for long-term wellbeing — is what happens in the hour after. The shame flood.
Within minutes of an episode ending, most people with IED enter a state of acute distress that can rival the intensity of the episode itself. The anger is gone. In its place is something more complex and harder to move through: deep shame, genuine confusion, grief about the relationship damage, and an overwhelming wish to undo what just happened. Research consistently shows that self-reported distress after IED episodes is high and that this post-episode shame is one of the strongest drivers of social withdrawal and secondary depression.
Shame operates differently from guilt. Guilt says 'I did a bad thing and I can make it right.' Shame says 'I am a bad thing and there is no repair.' People with IED who have not received psychoeducation about their condition are often stuck in a shame framework — every episode as further evidence that they are fundamentally dangerous, irreparably broken, undeserving of the relationships they have damaged. This internal narrative is both incredibly common and incredibly inaccurate.
The neurological event that produced the episode was not a moral failure. It was a timing mismatch in a brain that is differently wired. This does not remove the need for accountability — apology, repair, changed patterns over time. But it does mean the shame-as-identity framework is not only painful but counterproductive. Shame increases stress reactivity and threat sensitivity, which actually increases IED episode frequency. The shame cycle can perpetuate the very behaviour it is responding to.
Therapeutic approaches that work with IED consistently aim to replace shame-based self-appraisal with accountability-based self-appraisal: 'I had an episode. I am responsible for its effects. I have the capacity to learn and respond differently over time.' This is harder than it sounds when the shame is acute. It is also the pathway out.
Social withdrawal after episodes, while understandable, tends to prevent the relational repair that would actually reduce shame. Understanding the withdrawal pattern — and building, over time, a capacity to return and repair — is one of the most important skills in living well with IED.
- Post-episode shame is consistently rated as highly distressing and is a major driver of secondary depression in IED.
- Shame (I am bad) is less accurate and more harmful than guilt (I did a bad thing I can address).
- Shame increases stress reactivity, which can perpetuate the IED cycle rather than breaking it.
- Accountability-based self-appraisal — not shame-based — is the therapeutic pathway that actually reduces episodes.
Why Authority Triggers the IED Hair Trigger
Of all the consistent patterns in IED presentations, conflicts with authority figures are among the most reliably reported and the most consequential. Employers, teachers, parents, police officers, supervisors — any figure who holds structural power and uses it in a directive or corrective way can trigger explosive responses that damage careers, relationships, and legal standing with extraordinary swiftness.
Understanding why requires looking at how the IED threat-detection system processes perceived power dynamics. The amygdala, hyperreactive in IED, is particularly sensitive to signals of social threat — and in many people with IED, directive communication from an authority figure is processed as a dominance threat rather than neutral information. A supervisor saying 'I need this done differently' does not arrive as feedback. It arrives, neurologically, as an assertion of superiority with the implicit threat of social exclusion or punishment.
For people with histories of harsh discipline, unpredictable authority figures, or early experiences of genuine threat from power-holders, this sensitivity makes perfect evolutionary sense. The nervous system learned that authority can be dangerous and calibrated its threat response accordingly. The threshold for explosive defensive response to authority lowered because, at some point, that lowered threshold was protective.
In the present, this calibration misfires constantly. A reasonable management note. A teacher's correction. A police officer's instruction. These arrive through a nervous system that has learned to read them as attacks, and the response is proportionate to an attack — not to the actual event.
The hair-trigger response to authority also interacts with shame in a specific way. Correction from an authority figure often carries an implicit judgement (you did this wrong), and for people with high shame sensitivity — which is common in IED — judgement can activate threat responses as powerfully as physical threat. The explosion is not a tantrum. It is a defensive response to what is being processed as a serious threat to self-worth and social standing.
Therapeutic work with this pattern typically involves two tracks: desensitisation to the specific authority-trigger pattern through graduated exposure and cognitive reappraisal, and building skills to tolerate the discomfort of being corrected without activating the alarm system.
- The IED amygdala processes directive communication from authority figures as dominance threat rather than neutral information.
- For many with IED, this sensitivity has a history — early experiences with unpredictable or harsh authority calibrated the alarm threshold lower.
- Correction triggers shame, and shame can activate threat responses as powerfully as physical danger.
- Therapeutic work targets both desensitisation to authority cues and building tolerance for the discomfort of being corrected.
The Exaggerated Startle and What It Reveals
Exaggerated startle responses are so consistent in IED presentations that they function almost as a diagnostic marker in clinical practice. A sudden sound, unexpected physical contact, a sharp voice in a quiet room — and the person with IED doesn't just flinch. Their entire defensive system activates. Heart rate spikes. Muscles tense. Threat-scanning begins. And importantly, this activation doesn't resolve quickly. The echo persists.
The exaggerated startle in IED is a window into the baseline state of the nervous system. When the amygdala's threat-detection system is running at elevated sensitivity — as it does in IED — the threshold for triggering alarm is lower across all sensory channels. It's not that the loud noise is louder for someone with IED. It's that louder-than-expected sounds more readily cross the threshold into 'potential threat' territory, triggering a cascade of defensive physiological responses.
This persistent heightened startle is related to what researchers call hypervigilance — a chronic low-level scanning of the environment for threat. In people with IED, hypervigilance appears to be both a trait-level characteristic and a state-level response to accumulated stress. On high-stress days, the startle threshold drops even further. The system is already running hot, and very little input is needed to push it into explosive range.
The startle echo — that extended period after an unexpected stimulus where the nervous system remains elevated — is also significant. Many IED episodes do not follow a clear external trigger in the obvious sense. Instead, they follow an accumulation of these smaller startle-and-echo cycles throughout the day, each leaving the system slightly more activated, until a final (often small) trigger becomes the straw that tips it.
For people with IED, learning to monitor their overall nervous system activation state across the day — not just in the moment of explosion — is an important intervention. Recognising that you are running at 80% activation by 2pm (because of the morning commute, the difficult email, the noise at lunch) provides an early-warning context that purely reactive approaches miss entirely.
- Exaggerated startle in IED reflects a chronically lowered amygdala threshold for threat — not hypersensitivity to sound volume.
- The 'echo' after a startle keeps the nervous system elevated, creating an accumulation effect across the day.
- Many IED episodes follow accumulated smaller activations, not a single obvious trigger — tracking overall arousal across the day matters.
- Hypervigilance is both a trait-level characteristic in IED and a stress-sensitive state — high-stress days lower the explosion threshold further.
Amygdala Speed vs. Prefrontal Delay
The core neuroscience of IED can be summarised in a single number: 300 milliseconds. That is the approximate gap between when the amygdala generates its threat response and when the prefrontal cortex can apply modulation, context, and inhibition.
In a neurotypical brain, this gap is bridged by robust prefrontal-amygdala connectivity. The alarm fires (amygdala), but the prefrontal cortex almost simultaneously receives the signal and applies braking — context-checking, consequence-evaluation, impulse inhibition. The result is a threat response that is proportionate: real danger triggers real reaction; minor irritant triggers minor annoyance.
In IED, neuroimaging consistently shows two things: the amygdala is hyperreactive (fires earlier, fires more strongly to lower-threat stimuli) and the prefrontal-amygdala connectivity is reduced (the braking signal is weaker and arrives later). The gap that is 300ms in a neurotypical brain is effectively longer in IED — and in that extended gap, the explosive behaviour has already begun.
This timing mismatch is not fixed or permanent. Prefrontal-amygdala connectivity is modifiable through training, therapy, and in some cases medication. But it cannot be overcome in the moment of an episode by willpower alone, because willpower is itself a prefrontal function that is being outpaced by amygdala speed. Understanding this is critical: the failure point is at the timing gap, not at the 'desire to control oneself.'
Functional MRI studies of people with IED during provocation tasks show significantly greater amygdala activation compared to controls, and significantly less prefrontal activation during the same tasks. This is not metaphor. This is observable in brain imaging. The neurological difference is real, documented, and diagnosable — not a convenient excuse but a measurable biological phenomenon.
This understanding has therapeutic implications. The most effective interventions for IED target the period before the gap — building skills that engage the prefrontal cortex earlier in the cycle, so it has a chance of catching the amygdala response before the explosive behaviour is already underway.
- The amygdala fires 300ms before the prefrontal cortex can apply modulation — in IED, this gap is effectively longer.
- fMRI studies show measurably greater amygdala activation and less prefrontal activation during provocation in IED.
- Willpower is a prefrontal function — it cannot reliably intervene when the amygdala is operating faster than it can respond.
- The most effective interventions target the pre-gap period, engaging the prefrontal cortex before the alarm is fully activated.
How Serotonin Regulates Impulse Control
If the amygdala-prefrontal timing mismatch is the architecture of IED, serotonin is the fluid that keeps the braking system running. And in IED, the evidence consistently points toward a significant serotonin system difference.
Serotonin (5-hydroxytryptamine, or 5-HT) plays a central role in behavioural inhibition — the neural process by which an impulse is registered and then not acted upon. The serotonin system's role in aggression and impulse control has been studied for over four decades, and the association is robust: lower serotonergic function is consistently associated with greater impulsive aggression across species and across clinical populations.
In IED specifically, several lines of evidence converge. Cerebrospinal fluid studies show reduced 5-HIAA (a serotonin metabolite) in impulsively aggressive individuals. Genetic studies have identified variants in serotonin transporter and receptor genes (particularly 5-HT2A) that are overrepresented in IED. PET imaging studies show reduced serotonin receptor binding in frontolimbic circuits in people with IED compared to controls.
What this means in practice: the chemical system that normally signals 'suppress this impulse' is less active, less available, or less efficiently used in IED. When the amygdala generates a threat response and the body moves toward explosive action, serotonin is part of what normally applies the brakes. With reduced serotonergic function, those brakes are less effective — hence the 'missing brake fluid' metaphor.
This has implications for treatment. SSRIs (selective serotonin reuptake inhibitors) have shown efficacy in reducing IED episode frequency and severity in controlled trials. This is not because the medication 'calms people down' in a general sense — it is because increasing serotonergic availability in frontolimbic circuits specifically improves the impulse-inhibition function that is underperforming in IED. Understanding the mechanism helps destigmatise the medication: it is not a personality-changing chemical. It is topping up the brake fluid.
- Serotonin plays a central role in behavioural inhibition — reduced serotonergic function means less effective impulse braking.
- CSF, genetic, and PET imaging studies all converge on serotonin system differences in IED.
- Variants in the 5-HT2A serotonin receptor gene are overrepresented in IED populations.
- SSRIs show efficacy for IED because they top up the serotonergic brake system — not because they chemically suppress personality.
Reading the Body Before the Explosion
One of the most clinically significant and practically useful findings in IED research is this: 85% of people with IED report physical warning signs before an explosive episode. Tingling in the hands, a flush of heat across the face, tension in the jaw or chest, a specific quality of energy in the legs, a change in the quality of vision or hearing. These are real, consistent, and — crucially — they precede the explosion by several seconds to minutes.
This finding matters enormously because it means the 'no warning' narrative is incomplete. At the cognitive and emotional level, the explosion often does feel sudden and warning-free. But at the body level, there is a window. And that window is the primary access point for intervention in IED.
The challenge is that many people with IED have poor interoceptive awareness — difficulty registering and interpreting internal body signals. The very signals that could serve as early warning are not being consciously tracked. They arrive, escalate, and by the time the person becomes aware that something is happening, the cognitive tunnel has already narrowed.
Interoception training — systematically developing the ability to notice and interpret body sensations — is therefore a core component of evidence-based IED treatment. This is not about meditation or relaxation in the generic sense. It is about building specific awareness of your personal precursor signals, so that when you notice the heat in your face or the jaw tension, you have an automatic protocol ready: remove yourself from the situation, breathe into the signal, buy the 60 seconds your prefrontal cortex needs to catch up.
The 85% who have warning signals also need to know that these signals are learnable. Many people with IED spend years believing their episodes are completely beyond any warning. When they begin systematic body-scanning practice and discover that there IS a precursor state they had been missing, this is often experienced as genuinely transformative — not because it eliminates episodes immediately, but because it converts an experience of complete lack of agency into one with a small but real window of choice.
- 85% of people with IED report physical warning signs before episodes — the body knows before the mind catches on.
- Common precursors include facial heat, jaw or chest tension, tingling in the hands, and changes in sensory quality.
- Poor interoceptive awareness means these signals are often not consciously tracked — they arrive and escalate unseen.
- Interoception training — learning to read your specific precursor signals — converts 'no warning' into 'a small but real window of choice.'